
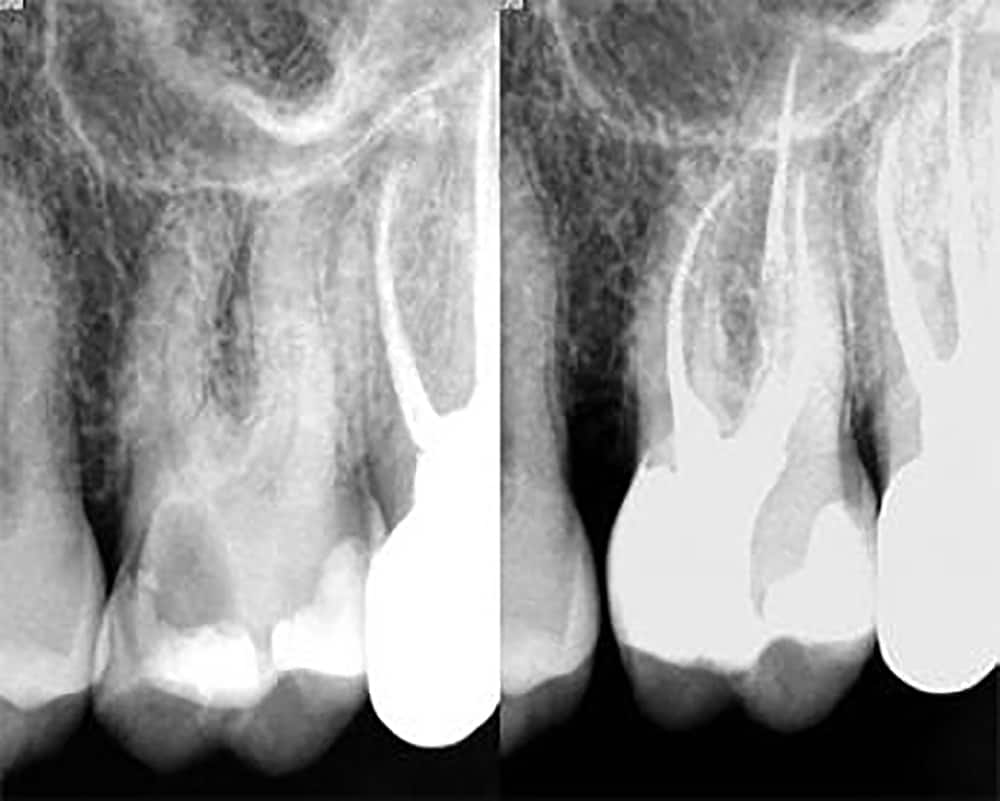
Endodontic Treatment (Vital/Non-Infected Teeth)
Dr. Soucie received his master’s thesis for his study of bacterial penetration of tooth structure. Vital teeth exhibiting irreversibly inflammation of the pulp (Ex. Lingering to hot/ cold) can be treated in a single visit due to the presence of intact blood and lymph vessels, primary components of our immune response that fights infections.
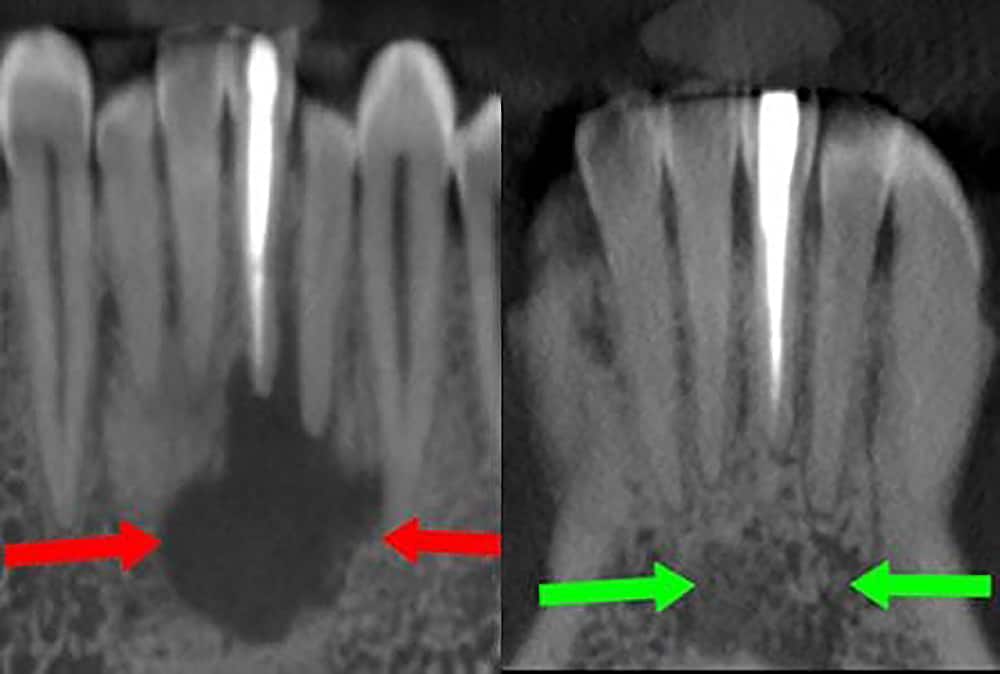
Microbiological Treatment
Necrotic teeth no longer possess viable pulp tissue to remove bacteria and become infected. Medicine is placed inside the tooth and left for several weeks. This works in concert with your immune system, facilitating bone healing which is requisite for completion of your treatment at Evolution Endodontics.
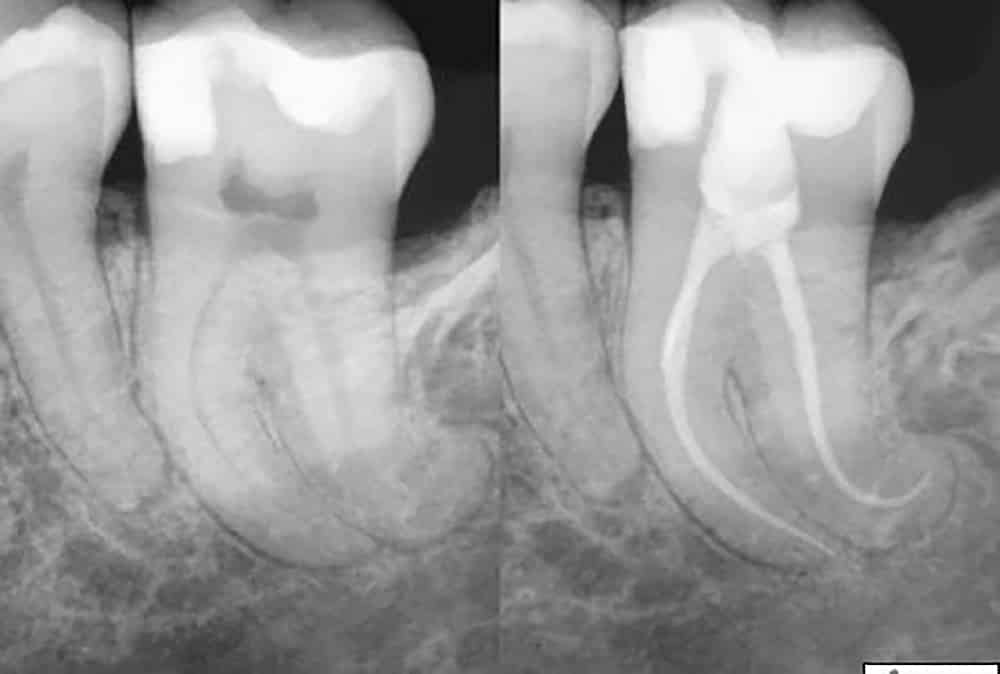
Endodontic Retreatment
Retreatment of failed root canals is due to bacteria presence, missed anatomy and incomplete removal of necrotic tissue. Therefore, the same microbiological protocol used on necrotic teeth is utilized to ensure increased treatment predictability and long term success.

Extraction/Socket Conversion
CT scans reveal accurate bone loss, fracture and internal anatomy. Non-restorable teeth are surgically extracted, bone graft and membranes are placed to facilitate eventual implant placement when desired. A follow up CT is taken 4 months later to ensure proper healing for implant placement. CT scans are sent to the appropriate party for implant placement and restorative therapy.

Dental Trauma
Replacement of displaced and avulsed (Knocked out) teeth and splinting of loose teeth. Root canal therapy and any required adjunctive therapy, such as the placement of posts and cores are performed. Crowns, when indicated, are performed by you general dentist or prosthodontist.
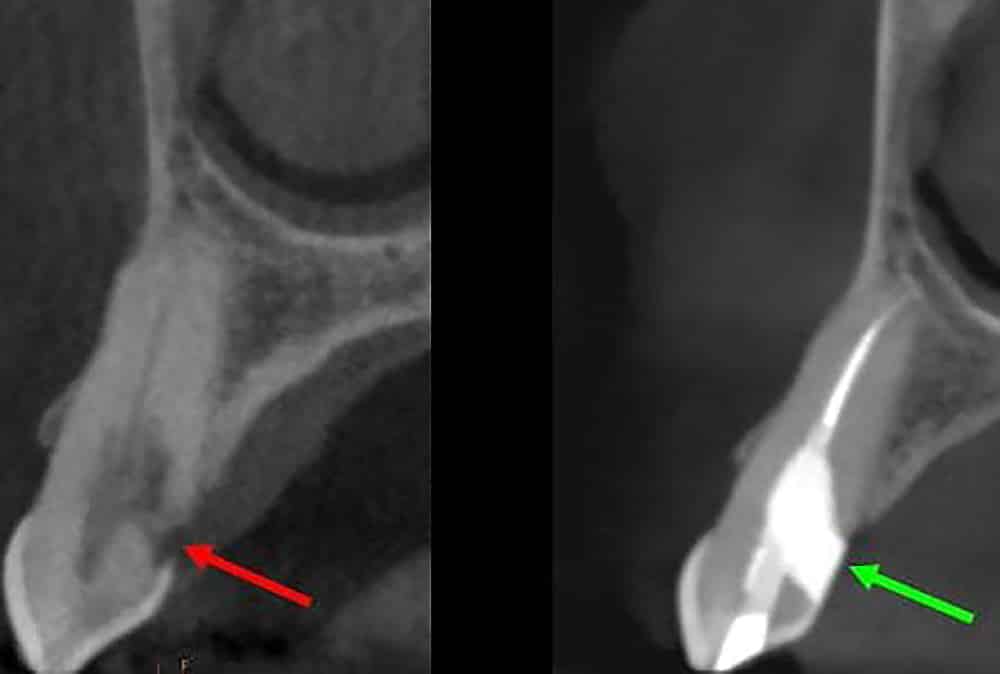
Resorption Therapy
Root resorption therapy is a viable treatment to eliminate the pathological process that results in the progressive loss of dentine and cementum by the action of osteoclasts. If left unnoticed or untreated, the resorptive lesion progresses and the effected teeth become non-salvagable and must be extracted.

Core & Post/ Core
A core is a type of dental restoration required to permanently restore an endodontically treated tooth when sufficient amounts of sound tooth structure remain to retain a conventional crown. A post and core is a type of dental restoration required when inadequate amounts of sound tooth tissue remain to retain a conventional crown. A post is cemented or bonded into a prepared root canal to retain a core restoration, enabling cementation and retention of the final crown. The post is analogous to rebar in concrete.

Root Resection/Amputation
Root amputation is a viable treatment to retain a functional portion of the tooth. Root amputation (root resection) is the surgical removal of all the root and adherent soft tissues leaving the crown of the tooth intact and supported by remaining root(s).

Apicoectomy
An apicoectomy is performed to eliminate the root end and associated infection, preserving the function of the tooth whilst avoiding extraction. This treatment is only considered when a root canal has failed and removal of restorative material, such as cast posts and crowns, would result in loss of the tooth.

Internal Bleaching
Internal bleaching is a conservative means of managing discolored teeth. The primary indication for internal bleaching is intrinsic (internal) discolouration, resulting from such things as trauma and bacteria. Contrary to external bleaching, internal bleaching is performed to brighten your teeth from the inside out. The objective of an internal bleaching lies in the removal of the tooth discoloration without sacrificing any hard tooth substance.
Crown Lengthening
During the dental crown lengthening procedure, excess gum and bone tissue is reshaped to expose more of the natural tooth. Perhaps your tooth is decayed, broken below the gum line, or has insufficient tooth structure for a restoration, such as a crown or bridge. Crown lengthening adjusts the gum and bone level to expose more of the tooth so it can be restored. This indication is consistent with the localized crown lengthening procedure that would be completed in addition to your restorative and endodontic procedures.
Left: Extensive decay extending subgingivally, proximal to the bone, and into the dental pulp
Right: Result following caries removal, crown lengthening, endodontic therapy and core build-up
 We Offer Laser Enhanced Root Canals with Increased Success Rate!
We Offer Laser Enhanced Root Canals with Increased Success Rate!